Surgical Treatment
Patients with symptomatic gallstones and with or without the complications are advised by their physicians to undergo surgery to remove the gallbladder. Two types of surgeries are available laparoscopic cholecystectomy commonly referred to as keyhole surgery and open cholecystectomy. The patient is first admitted to the hospital, then routine blood tests are carried out and then the patient is prepared for the surgery by making him NPO (nil per oral) i.e. no food or drink is allowed from 8- 12 hours prior to the surgery, and prophylactic antibiotics are given.
Laparoscopic Cholecystectomy
Laparoscopic cholecystectomy or more commonly referred as lap choly is the most commonly used surgical approach. It was first used in 1987 and since then its popularity has increased, replacing the conventional open cholecystectomy.
The advantages of the procedure are that it requires a short hospital stay, lesser time to recover and the surgical incisions are healed quickly. The disadvantage is that for very obese patients it is not recommended because visualising the internal organs through a thick layer of fat is quite difficult and also that when placing the surgical instruments there might occur some injury to the abdominal contents.
- The procedure starts with anaesthetizing the patient.
- Then using insufflation needle a pneumo peritoneum is created i.e. the abdominal cavity is distended or made bigger by pumping carbon dioxide through a needle, so that the abdomen can be visualised clearly on the monitor.
- Four small incisions are given, one in the umbilicus for the passage of endoscope and three incisions or ports are created on the right side of the abdomen for the passage of surgical instrument.
- The surgeon then finds the cystic artery and cystic duct, divides it into half by stapling or clipping or ligating them, so that there is no leakage of the bile from the duct into the abdomen and no blood loss from the artery.
- After dividing and closing the duct and the artery, the gallbladder is finally removed as a whole from one of the ports usually from the umbilical port.
- The incisions are then closed with sutures or sticthes.
The advantages of the procedure are that it requires a short hospital stay, lesser time to recover and the surgical incisions are healed quickly. The disadvantage is that for very obese patients it is not recommended because visualising the internal organs through a thick layer of fat is quite difficult and also that when placing the surgical instruments there might occur some injury to the abdominal contents.
Open Cholecystectomy
This procedure was used widely until the early nineties, when it was gradually replaced by lap choly. It is still used today in about 5% of the cases; where for some reason lap choly cannot be undertaken, for e.g. in patients who have had extensive previous abdominal surgery and in patients with complications of acute cholecystitis (empyema, gangrene or perforation of the gallbladder). About 5-10% of the laparoscopies are converted to open cholecystectomy during the procedure itself due to various reasons such as:
The procedure is just as same as that of lap choly, with the difference being in the type of incision given and no air or gas infusion is requires due to wide excision. The excision given is either a large para-median (near the midline, vertically) or a right subcostal (below the ribs) called the Kocher’s incision is given. The rest of the procedure is the same.
The advantage of this procedure is that abdominal structures are clearly visualised and thus reduces any chance of injury. If gallstones are suspected in the bile ducts then X- rays are taken on the spot and can be taken out. The disadvantages of the procedure are that it takes a longer stay in the hospital and the recovery time is also increased.
- An injury to the major blood vessel.
- The internal structures are not clearly visualised.
- Deviation from the normal human anatomy.
- A thickened gallbladder wall due to inflammation.
- When the stones from the common bile duct cannot be removed with laparoscopy or ERCP.
The procedure is just as same as that of lap choly, with the difference being in the type of incision given and no air or gas infusion is requires due to wide excision. The excision given is either a large para-median (near the midline, vertically) or a right subcostal (below the ribs) called the Kocher’s incision is given. The rest of the procedure is the same.
The advantage of this procedure is that abdominal structures are clearly visualised and thus reduces any chance of injury. If gallstones are suspected in the bile ducts then X- rays are taken on the spot and can be taken out. The disadvantages of the procedure are that it takes a longer stay in the hospital and the recovery time is also increased.
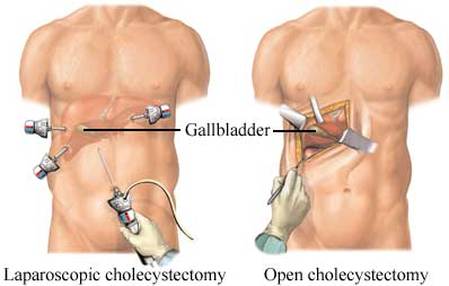
Fig.11 Difference in size and incision sites between lap choly and open cholecystectomy. n.d. [online] Available at: < http://www.beliefnet.com/healthandhealing/getcontent.aspx?cid=42694> [Accessed 12 May 2013]
